BACKGROUND: To date, surgical treatment is an effective treatment of hypercortisolism in primary bilateral macronodular hyperplasia (PBMAH). Due to the bilateral lesion, the most common treatment in Russia is the bilateral adrenalectomy, which requires the appointment of hormone replacement therapy. The results of various studies on the effectiveness of unilateral adrenalectomy (UA) in PBMAH are rather discordant.
AIM: The objective of the study was to assess the outcomes of UA in patients with PBMAH, accompanied by mild autonomous cortisol excess (MACE) or overt Cushing’s syndrome (CS).
MATERIALS AND METHODS: 44 patients with PBMAH and a manifest form of CS (n=21) MACE with comorbid conditions (n=23) underwent UA in the surgical department of the Endocrinology Research Centre. The dynamics of laboratory parameters (cortisol after overnight dexamethasone suppression test (cortisol ONDST) urinary free cortisol (СКМ), ACTH), as well as the course of comorbid diseases (diabetes mellitus, arterial hypertension (AH), metabolic disorders) were assessed before and after 6 months of surgical intervention. The cut-off level of blood cortisol (8:00–9:00) during the first day after OA was determined as a predictor of the development of adrenal insufficiency (AI) in the early postoperative period.
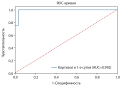
RESULTS: 6 months after OA, laboratory parameters improved in 40/44 (91%, 95% CI: 78%-97%) cases: cortisol ONDST decreased from 466 [173; 652] to 86 [61; 149] nmol/l, p=<0.01, СКМ dropped from 840 [468; 1892] to 267 [204; 432] nmol/day, p=<0.01), while ACTH increased gradually from 1 [1; 2.1] to 8.3 [2.6; 15.0] pg/ml, p=<0.01), which indicates the effectiveness of UA. Statistically significant changes in BMI were also obtained (before UA — 30.8 [27.5; 34.4], after — 28.5 [23.9; 32.2] kg/m2 (p <0.01)). When analyzing the long-term outcomes of UA on carbohydrate metabolism, a decrease in the level of HbA1c from 7.0 [6.3; 7.7] to 6.0 [5.6; 6.7] %, (p<0.01) was observed. Further, there was an improvement in the course of AH. After UA, antihypertensive therapy was completely discontinued in 27.7% of cases, and a reduction in the number of antihypertensive drugs was carried out in 44.4%. The level of cortisol in the early postoperative period less than 325 nmol/l was the strongest factor predicting the potential adrenal failure (AUC=0.96).
CONCLUSION: UA can be recommended as the first line treatment of PBMAH with CS due to the high probability of longterm remission of hypercortisolism and improvement in the course of comorbid diseases.