


Clinical lecture

This lecture presents 3 methods of thyroidectomy; the most common and widely used thyroidectomy method, i.e. the extrafascial thyroidectomy method (1), the historical subcapsular thyroidectomy method (2) and the combined extrafascial and subfascial thyroidectomy methods (3). Each of these methods is used in everyday practice and have their own indications for use. The methods are presented with a detailed description of the steps. In the description of the technique of the operation, we determined the stages. The presented three methods of thyroidectomy are a systematization of the existing widely used surgical methods of operation for various diseases of the thyroid gland. In our opinion, this systematic step-by-step approach to thyroidectomy, taking into account the characteristics of thyroid pathology, can improve the standards of treatment, surgical outcomes and training of surgeons in the field of thyroid surgery.
Original study
Background: Diabetes mellitus (DM) is one of the most common chronic diseases, leading to the development of many complications includingdiabetic foot syndrome (DFS). The problem of a progressive increase in the number of patients with DFS and the high risk of amputation in the population of patients with DM requires research to identify risk factors and specify ways to correct them.
Aim: To study the clinical and laboratory characteristics of patients of the limb rescue center suffering from type 2 diabetes (DM2).
Materials and Methods: A retrospective analysis of 729 medical histories of patients with T2D hospitalized in the foot rescue department of the limb rescue center of the State Clinical Hospital named after V.P. Demikhov in the period between 2019 and 2020 was carried out. An analysis of anamnestic data, clinical and laboratory parameters, drug therapy, the nature of surgical intervention and the outcome of hospitalization was performed. The statistical analysis was carried out using STATISTICA 8.0.
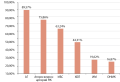
Results: The study included 729 patients with T2D. Men dominated among patients (58%). The median of age was 66 [59.0; 73.0] years. 50.89% had experience of diabetes for more than 10 years. 53% of these patients had DFS, 79.2% had diabetic polyneuropathy, 45% had previously undergone amputation of the lower extremity, 24.8% had revascularization. A significant proportion of patients at admission had uncontrolled high level of glycemia. The median of glucose level was 9.9 mmol/l [7.2; 13.8]. Median meaning of HbA1c was 7.8% [6.7; 9.1]. BMI and lipid profile were not evaluated in all patients. In the department 224 patients were diagnosed with DFS for the first time. Gangrene prevailed among the ulcerative-necrotic complications of DFS. Arterial hypertension (AH) prevailed among the concomitant pathologies. GFR ˂ 60 ml/min/1.73m2 was observed in 45.36% of patients. According to X-ray data, 27.16% of patients (107 out of 394) showed signs of impaired bone density. In the department, 113 patients underwent revascularization, 372 — amputation of the lower limb, while 37 patients (9.95%) underwent amputation at the level above the knee, and 335 (90.05%) — at the level below the knee. Only 244 patients received local treatment among patients with DFS. A total of 718 patients were discharged; 11 patients died. The median duration of hospitalization of discharged patients was 13.0 [9.0; 18.0] bed days, the average duration of hospitalization of deceased patients was 11.31±2.21 (95% CI 6.49–16.13) bed days.
Conclusion: Most of the patients with DM2 and DFS had prolonged decompensation of carbohydrate metabolism, dyslipidemia, increased BMI, hypertension. The study concluded that it is important to monitor and correct risk factors to improve the prognosis of the disease.
Endocrine oncology
Obituary


This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0).
ISSN 2310-3965 (Online)




































